Catapult Education Product Review
SDI Riva Star Aqua

A New Approach to Class II Lesions
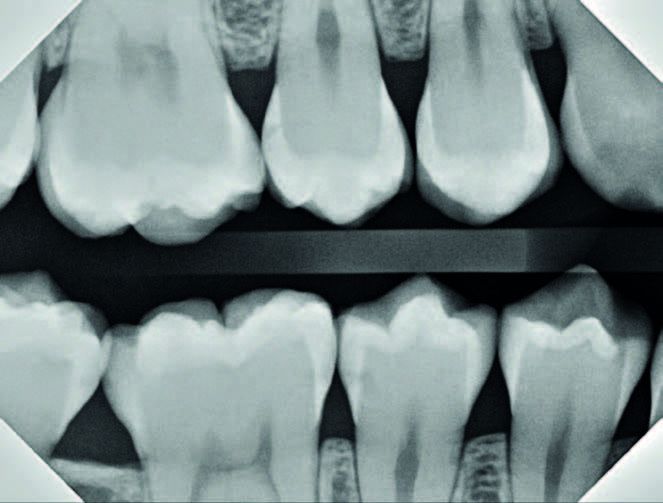
The way I was taught to treat class II lesions is antiquated, unpredictable, and barbaric. Take a look at the bitewings in [Figure 1].
Take your time. I’ll wait.

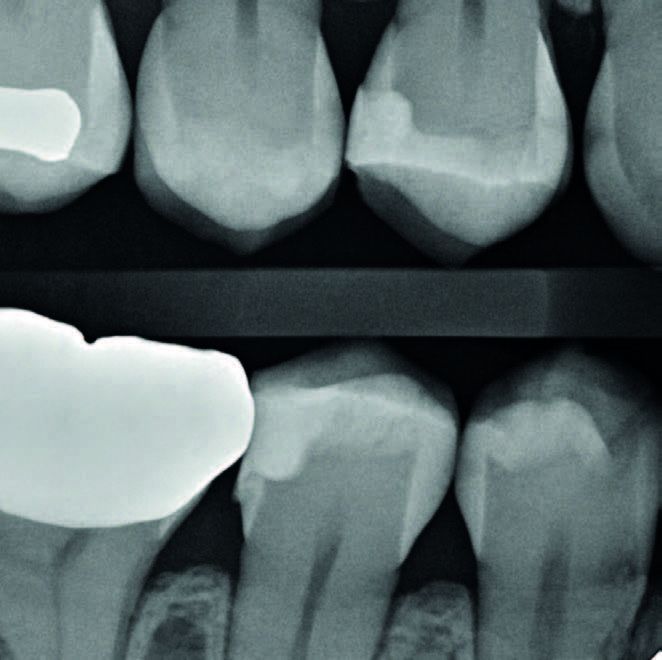
If you are anything like me, you would have recommended some watches, and some class II fillings. That’s what I did for over 20 years. And I now really regret it. Sadly, for a variety of reasons, neither is a great option. First, drilling is barbaric, destructive, and incredibly invasive. Let’s zoom in on the anterior right radiograph [Figure 2].
More than likely, the majority of you believe that #4, #29, #30 and #31 require some kind of intervention. At the very least, they shouldn’t be completely ignored. If you received your dental training similar to mine (I graduated from the University of Michigan in 2004), then it is within the realm of possibility that you would recommend quite a few MOs and DOs, maybe even an MOD for #30.
In order to adequately remove all the decay for all of these restorations, you would have to, access the interproximal surface via an occlusal prep; break all interproximal contact in order to place a band; bevel cavosurface enamel; round any sharp angles between the walls in the proximal box.
All of those steps involve destruction of healthy enamel and dentin. Your prep would end up looking something like [Figure 3]. Relative to the size of the cavity, that is a lot of enamel destruction.
Even setting aside the lost enamel, class II composite cases are difficult. The proximal box must be sealed, an adequate contact must be reestablished, the filling must exhibit smooth interproximal margins, and the entire body of the filling has to be free of voids. Yes, sometimes the sectional matrix band, wedge, and ring just fit perfectly, but sometimes they don’t. Sometimes the ring pops off, or the band doesn’t quite seal and you end up with a restoration that looks like [Figure 4].
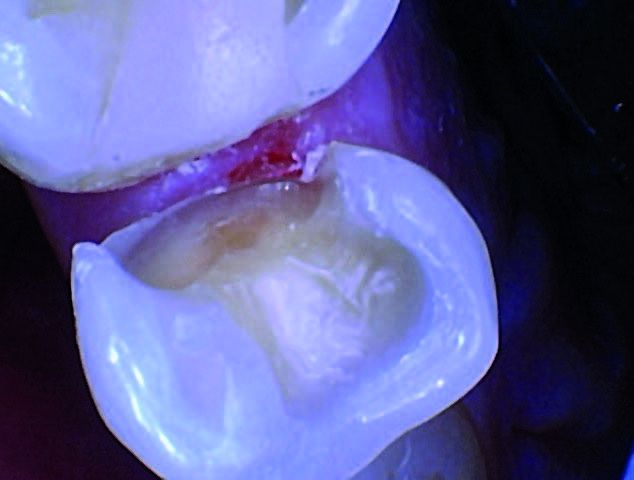
This can be demoralizing. As a dentist, I know their interproximal cavity was so small to begin with, and I have to ask if I made things better or worse by doing the restoration? Another question I ask is would we do the same class II restoration on ourselves?
I believe there is an equal amount of inadequacies with the “watching” technique because it provides no solution. The inevitable is delayed, which is nice, but as dentists who practice in the midst of so much technological innovation, we could do better.
Most dentists now understand that silver diamine fluoride (SDF) is a highly effective “arrester” of decay. To this point, its major contribution to the field of dentistry has been as a solution for low-income individuals with rampant decay. Because of the potential financial inability for these individuals to undergo traditional dental solutions such as fillings, instead they are offered SDF application so that the cavities don’t get worse. This solution has not been widely accepted outside the realm of low-income clinics, however, because of the highly unpleasant side effect of SDF turning the tooth black.
A new approach

Congratulations: SDI Riva Star Aqua
Learn More about SDI
Products for Your Patients
Say NO to boring CE.
new on-demand and LIVE online courses!